 |
|
|
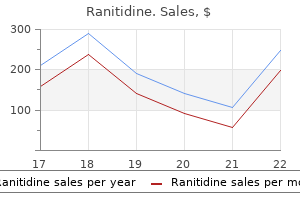
Ranitidine dosages: 300 mg, 150 mg
Order ranitidine 150 mg with visaA gastritis diet 91303 effective ranitidine 150 mg, the characteristic "dewdrop on a rose petal" is illustrated by this early vesicle on an erythematous base gastritis help ranitidine 300 mg order fast delivery. B, the standard features of lesions in all levels of evolution is seen on the trunk of this baby. Note the presence of papules, vesicles, and umbilicated and scabbed lesions, all within a small space. C and D, In this youngster with underlying eczema, the primary crop of vesicles appeared in clusters at sites beforehand affected by dermatitis. The flexor surface of his arm is roofed with quite a few discrete lesions, and vesicles are confluent over the plantar surface of his toes and on the balls of his ft. E, On mucosal surfaces, thin-walled vesicles may form and quickly rupture, forming painful shallow ulcers. A delicate prodrome consisting of low-grade fever and malaise is typical and may be related to generalized adenopathy, hepatosplenomegaly (especially with hepatitis B), upper respiratory tract signs, or diarrhea. The exanthem typically clears inside 2 to three weeks however can persist for eight weeks or extra. Bacterial Exanthems Streptococcal Scarlet Fever Although mostly associated with pharyngitis and impetigo, S. B, In the immunocompromised youngster, pores and skin lesions are inclined to be hemorrhagic and almost confluent. C, Lesions also evolve more slowly than ordinary, remaining vesicular for a protracted period. Vesicles coalesce over a quantity of days (B), and lesions then evolve to a crusted stage (C). D, Involvement of the ophthalmic department of the trigeminal nerve produces lesions involving the forehead, eyelids, and nostril. A and B, Lesions consist of raised lichenoid papules with flat tops that appear in crops and tend to remain discrete. C, this youngster reveals the characteristic acral distribution, with lesions involving the extremities and face but with relative sparing of the trunk. Transmission requires close contact to allow the direct unfold of large droplets. The incubation period for scarlet fever ranges from 12 hours to approximately 7 days. The disease is contagious in the course of the acute interval, and sufferers may transmit the organisms throughout energetic subclinical infection as nicely. An average of 50% of relations dwelling with an index case become secondarily contaminated, and up to half of those have subclinical disease. Once a severe sickness associated with high morbidity and mortality, scarlet fever has turn into a much milder illness over the past several many years. The traditional presentation consists of the abrupt onset of fever, chills, malaise, headache, sore throat, and vomiting; abdominal pain additionally could also be a prominent criticism. Within 12 to 48 hours, an exanthem appears and quickly generalizes, normally beginning on the trunk and spreading peripherally, but typically spreading cephalocaudally, complicated this with measles. The remaining skin becomes diffusely erythematous and is roofed by tiny pinhead-sized papules, with a sunburn look of erythroderma. Examination of the oropharynx in basic circumstances reveals giant, erythematous and exudative tonsils, together with palatal erythema and petechiae (see Chapter 24). Without treatment, the rash, fever, and pharyngitis resolve within 1 week; with treatment, improvement is extra fast inside days. Diagnosis is straightforward in classic instances, however the extensive spectrum of disease severity and potential manifestations could trigger confusion. A and B, In the classic form of this exanthem, the patient has a flushed face, perioral pallor, and a diffuse, blanching, erythematous rash that has a sandpapery consistency on palpation. D, During the first 1 to 2 days the tongue has a white coating through which outstanding erythematous papillae project-a white strawberry tongue. E, A few days later the white coat peels, leaving the attribute pink strawberry tongue with glistening floor and distinguished papillae. F and G, Desquamation occurs in fine, skinny flakes because the acute phase of the sickness resolves and is proportional to the depth of the exanthem. In this child with streptococcal scarlet fever, the rash has a patchy distribution but is accentuated within the axillae and different creases. Pharyngitis may be mild (without exudate, petechiae, or marked erythema) or absent, even when the throat is the site of infection. If streptococcal pores and skin or wound infections are the first site of infection, the oropharynx is regular. Still others could present with fever or nasopharyngitis and urticaria as their initial manifestations. In dark-skinned kids, erythema and perioral pallor could also be difficult to appreciate and the papules could additionally be larger, thus producing a texture much less like that of sandpaper. A, this toddler reveals proof of epidermal separation and has numerous ruptured bullae over the inguinal area and thighs. B, In this older baby, symptoms have been mild and solely the pores and skin of the face, axillae, and perineum showed indicators of epidermal separation. Note the proof of a positive Nikolsky sign on her higher lip and cheek, the results of wiping her nostril. C, A denuded area is clear on the higher chest, and thick flakes have begun to kind on the face of this infant. Therefore, in sufferers with fever or nasopharyngitis and urticaria and in youngsters with scarlatiniform eruptions, a screening throat culture for S. Sites of carriage embrace the nose, gastrointestinal tract skin, perineum, and nails. In every illness, organisms on the primary website of infection launch distinct superantigen exotoxins, which then produce the associated rash. Draining pores and skin lesions, nasal discharge, and contaminated palms constitute significantly necessary sources of transmission. Traumatic or surgical wounds, burns, insect bites, areas of preexisting dermatitis, viral pores and skin lesions, and prior viral respiratory tract infection all function predisposing conditions. Staphylococcal Scalded Skin Syndrome A dysfunction seen mostly in infants and younger youngsters, staphylococcal scalded skin syndrome is caused by exfoliative toxinproducing strains of S. The main infection is normally gentle, with purulent nasopharyngitis, conjunctivitis, impetigo, and infections of the umbilicus and circumcision sites seen mostly. Rarely, sepsis, pneumonia, or other severe invasive staphylococcal infections might precede the onset of the exanthem. After an infection, exfoliative toxin is spread hematogenously and causes cleavage of the skin between the dermis and the dermis. This process may start within hours or days of the appearance of indicators of the primary an infection, and sometimes its onset is heralded by fever and irritability, usually accompanied by vomiting. These symptoms are followed by the development of a diffuse, sunburn-like erythroderma that spreads rapidly from head to toe. In contrast to streptococcal scarlet fever, the concerned skin is tender, even to mild contact. During this part, software of sunshine traction on the pores and skin pulls dermis away from dermis, leaving a uncooked, weeping floor. Syndromes
150 mg ranitidine cheap with amexToxic granulations and a D�hle physique are found within the blood of this baby with sepsis chronic gastritis flare up 300 mg ranitidine cheap visa. The D�hle physique appears as a grayish-blue staining area gastritis diet óêðçàë³çíèöÿ ranitidine 150 mg discount line, which is situated on the inferior border of this cell. Atypical lymphocytes within the peripheral blood are often observed in sufferers with infectious mononucleosis. Peripheral blood smear showing an Auer rod (red, rod-shaped determine within the cytoplasm) inside a myeloblast of a patient with acute nonlymphocytic/acute myelogenous leukemia. These lymphoblasts are bigger and extra heterogeneous in look than L1 lymphoblasts. In addition, the nuclearto-cytoplasmic ratio is decrease, and nucleoli more distinguished, than in L1 lymphoblasts. Additional manifestations of this disorder embody hepatosplenomegaly and circulating myeloblasts. However, 20% to 30% of sufferers with Down syndrome and transient myeloproliferative disorder develop leukemia within the first 3 years of life. Bone Marrow Failure Pancytopenia refers to a reduction in all three shaped components of the blood. Pancytopenia could happen from bone marrow failure or extramedullary mobile destruction (as seen in autoimmune disease, significantly systemic lupus erythematosus) or as a mix of depressed marrow function and increased cellular destruction. On the opposite hand, the pancytopenia ensuing from bone marrow failure could be divided into genetically predisposed marrow failure syndromes and acquired marrow failure syndromes. Aplastic anemia is marked by peripheral blood pancytopenia related to bone marrow hypocellularity or acellularity. Acquired aplastic anemia is an immune-mediated disease, although genetic risk factors and environmental exposures doubtless contribute. Research has resulted in a much deeper understanding of the function that activated T lymphocytes play in presenting hematopoietic cell antigens for destruction. In youngsters, the acuity of presentation in aplastic anemia relates to the degree of pancytopenia. Severe aplastic anemia is assessed as a bone marrow pattern that demonstrates less than 25% cellularity, in association with peripheral cytopenias in two of the three lineages. Pancytopenia is a common presentation for each Fanconi anemia (a chromosomal breakage syndrome) and dyskeratosis congenita (a telomere size disorder). Fragility of the chromosomes and pancytopenia, nevertheless, can happen within the absence of physical anomalies. Its pathophysiology is greatest regarded as an uncontrolled cytokine storm and is due to abnormalities of the antigen-presenting and antigen-processing histiocytes. International research research and consensus panels have led to newly revised suggested standards (Table 12. However, with chemotherapy and bone marrow transplantation, outcomes have improved greatly. However, it remains a big contributor to the morbidity and mortality of childhood diseases. More than 10,000 new instances of cancer are identified throughout childhood within the United States each year. The capacity to deal with and remedy childhood malignancies has improved dramatically over the past few decades, which is encouraging. This is due, in massive part, to advances made in cooperative group scientific trials, the introduction of novel chemotherapy agents, and enhancements in supportive look after the patient receiving chemotherapy. In the 12 months 2010, an estimated 1 in 500 people between 15 and 45 years old is a survivor of childhood cancer. This diagnosis should be considered if the rash is unusually extreme or persists regardless of standard treatment measures. Additional bodily examination findings that should enhance the suspicion for this analysis embody any erythema of gingival mucosa, organomegaly, or systemic signs, similar to irritability or failure to thrive (see Chapter 8). B and C, Hemorrhagic and papular rashes are additionally seen in some children with this disease. The initial task of recognizing the signs and symptoms of malignancy normally falls to the pediatrician, family medicine doctor, or emergency room doctor. The present part aims to evaluate medical displays that ought to alert the physician to the potential of a malignant process. As with most pediatric situations, the differential analysis varies relying on the age of the kid. An immediate concern at the time of prognosis is to prevent any tumorrelated complications, including neutropenia due to marrow infiltration, metabolic abnormalities because of increased cell turnover, or organ compromise due to space occupying lesions. Signs and symptoms of the most common tumors of childhood are reviewed in a manner that parallels the physical examination. This methodology might lead to a point of overlap, as a result of many cancers manifest a wide spectrum of displays that will differ in location within the body. Each tumor subtype is mentioned within the context of a area by which it sometimes presents. Signs and Symptoms Red flags that signal malignancy may be detected in the midst of historical past taking and physical examination or in primary laboratory testing. Alternatively, the fast cell division could lead to metabolic abnormalities, including hyperkalemia, hyperuricemia, and hyperphosphatemia with reflex hypocalcemia as a manifestation of tumor lysis. Opsoclonus�myoclonus Ataxia syndrome (random eye movements, myoclonic jerking and ataxia) tends to occur in patients with low-stage illness and favorable histology of the tumor. Unfortunately, many are left with devastating developmental and neurocognitive deficits that relate to this rare paraneoplastic situation. Even rarer is Kerner-Morrison syndrome, by which the affected person experiences intractable secretory diarrhea, hypokalemia, and dehydration. This situation represents the secretion of vasoactive intestinal peptide and has additionally been described in patients with neuroblastoma. The baby with a brand new analysis of malignancy is typically asymptomatic, which may be the case in a baby with a palpable stomach mass. In other instances, nonspecific signs could also be a prominent discovering, including fever, weight loss, and/or lethargy. Examples of more specific signs and signs in pediatric malignancy include the following: headache and morning vomiting in a affected person with a mind tumor; constipation and difficulty voiding in a patient with a pelvic tumor or spinal twine compression; hypertension in a child with a renal or suprarenal tumor; bone pain and limping in a young child secondary to leukemia; or, much less generally, another marrow-infiltrative course of. However, persistence (2 weeks is an affordable guideline) or undue severity might give these signs increased significance. Similarly, within the context of a selection of predisposing, underlying ailments, malignancy must be considered earlier. Children with a historical past of 1 cancer, by advantage of genetics or as a long-term aspect effect of anticancer remedy, are at larger risk of a second cancer. For instance, radiation therapy predisposes to a lifelong increased risk of strong tumors throughout the radiation area. The notable exception is the toddler or toddler who has an identical twin with leukemia. In this child, the risk of leukemia could also be as high as 25% in the first few years of life. Ranitidine 300 mg buy discount on-lineAlthough the cleft may be a component of an identifiable syndrome gastritis diet 100 discount 150 mg ranitidine free shipping, it more commonly happens as a solitary nonsyndromic defect gastritis medication buy ranitidine 300 mg low cost. Facial clefting is frequently categorized into cleft lip with or with out cleft palate and the isolated cleft palate. Epidemiologically, a distinction is notable between the 2 with respect to incidence, race, and sex. Approximately 1 in seven hundred reside births is affected with a cleft lip with or without cleft palate, occurring twice as typically in males. Asians represent the biggest population of affected infants, followed by the white population, and then African Americans. Cleft palate has a lower incidence of roughly 1 in one thousand live births, with barely more females affected, however no ethnic predilection. Embryologically, at the finish of the fifth week the maxillary prominences develop medially, and the medial nasal prominences are displaced towards the midline, where they fuse and ultimately form the premaxilla, which contains the philtrum of the higher lip, the portion Table23. Simultaneously, maxillary prominences develop outgrowths called the palatine cabinets, which fuse in the midline, forming the secondary (posterior) palate. The primary and secondary palates be part of on the incisive foramen to separate the nasal and oral cavities. During this weak period, anatomic interference (malposition of the tongue because of mandibular hypoplasia, as in Pierre Robin sequence), miscues in cell differentiation and migration, or teratogens (phenytoin, retinoids, steroids, lithium, and maternal smoking) might result in clefting in the developing fetus. Initial difficulties develop from the lack of the toddler to create an hermetic seal to suckle effectively, which is related to the scale of the clefts. Upright positioning and adaptive feeding nipples can help with stopping regurgitation and achieving effective closure around the nipple to acquire a seal. Breastfeeding is feasible for some infants with clefting; in fact, as a end result of the breast is more compliant, the infant might fare better in creating a seal around the breast. Cleft palates lead to disruption of the muscular levator veli palatini and tensor veli palatine slings, which might disrupt eustachian tube air flow and result in frequent bouts of otitis media. Persistent effusions might end in conductive hearing loss with subsequent delays in speech and language growth. Careful monitoring of middle ear effusions is crucial and the position of tympanostomy tubes by the pediatric otolaryngologist is commonly required to allow adequate drainage. Indeed, listening to loss may be identified in up to one-third of youngsters with palatal clefting, underscoring the importance of continued audiology surveillance by way of adulthood. Plastic surgical procedure reconstruction of facial clefts is a multistep endeavor, depending on the type and diploma of deformity. The objectives are aesthetic enchancment, upkeep of regular maxillofacial progress, and restoration of palatal perform in an effort to assist normal phonation. Reparative methods proceed to evolve, and controversy exists as to optimum timing and optimum process. For extensive unilateral and bilateral clefts, most centers will preoperatively slender the cleft to obtain higher outcomes. Some centers carry out a lip adhesion, or simpler approximation of the defect, when the infant is younger than three months old; others preoperatively slender the cleft defect by presurgical orthopedics, or personalized intraoral mouth/nosepieces adjusted by pediatric orthodontists. A, Left-sided unilateral cleft lip with minimal gentle tissue involvement or "forme fruste. In some facilities, palate repair may be combined with the preliminary lip repair, but in most the palate restore is performed several months later, from 9 to 12 months old. Optimal hearing and speech acquisition evolve when palatal integrity is restored earlier than the second birthday. As such, palate closure is often performed before 2 years old despite considerations that early surgical interventions involving the midface may have a negative impression on maxillofacial development and end in midface retrusion. Studies continue to try to define intervals when palatal procedures could be carried out with a minimal of untoward results. Unique errors of speech articulation are frequent to patients with cleft palate and usually have a tendency to develop in kids who undergo delayed palatal repair. Hypernasal speech, also known as velopharyngeal insufficiency, might occur in sufferers in whom the soft palate is foreshortened and permits air to escape into the posterior nasal vestibule. For these sufferers, a pharyngeal flap procedure could additionally be carried out whereby a peninsula of the posterior pharynx is connected to the taste bud. This recruited tissue serves to lengthen the palate and considerably alleviates hypernasal speech. Between ages 7 and 10, in the course of the time of combined dentition, an alveolar bone graft is usually indicated to permit regular eruption of the canine on the affected side(s), as well as to restore the maxillary arch, present nasal help, and shut the alveolar cleft. At this time, residual nasal deformities, which normally contain a broad and inferiorly displaced nasal ala, could also be focused by a proper rhinoplasty. Malalignment of the upper and decrease jaws may additionally exist due to deficient maxillary progress. Once mandibular growth is complete, surgical advancement of the midface could be carried out to restore regular occlusion. As this transient dialogue outlines, the family of a new child with a facial cleft can anticipate numerous procedures spanning the entire childhood of their toddler earlier than reaching the top of the restorative journey. Deformational Plagiocephaly the overall term plagiocephaly, derived from the Greek word plagio which means "oblique," describes an uneven skull. Etiologies can be intrinsic, such as genetic elements causing untimely suture synostosis, or extrinsic, similar to mechanical factors in utero or postnatally. About 10% of cases are congenital, from pressure causes similar to a number of gestations or lowered maternal pelvic quantity. Postnatally, occipital flattening is acquired from persistent supine sleep positions. In truth, compliance rates with the "Safe to Sleep" campaign correlate with the incidence of deformational plagiocephaly, with the white inhabitants affected essentially the most, followed by African Americans and Hispanics. Other related factors are male gender, multiparity, and torticollis, of which the latter is related to up to 20% of infants with deformational plagiocephaly. Right-sided deformational plagiocephaly is extra widespread, probably as a end result of right-handed moms holding infants in a Positional molding right-side-down position to nurse, inflicting stress and flattening of the proper occiput. Regardless of the facet, as quickly as a preferential supine place develops, it becomes recurring and troublesome to correct. History often confirms a normal head at birth and purchased asymmetry that worsens with time. Posteriorly, the mastoid skull bases ought to be symmetric; otherwise, there could be suspicion for a true unilateral lambdoid synostosis, described later. Whenever not sleeping, infants must be placed inclined ("tummy time") to decrease preferential supine positioning and to increase shoulder girdle strength. Changing the position of stimuli within the crib can also influence the infant to turn to a unique aspect. Although a rolled-up towel or foam pinned to the clothes on one facet will stop the infant from sleeping on that facet, care have to be exercised to avoid supplies in cribs that pose dangers to the sleeping infant.
Generic ranitidine 300 mgKey Knowledge Gaps � the optimum noninvasive tests for nonalcoholic fatty liver illness and alcoholic liver illness stay to be determined gastritis symptoms spanish ranitidine 300 mg buy visa. Conclusion Noninvasive testing is now a clinically recognized possibility for the analysis of liver fibrosis and has modified the diagnostic method to staging liver illness diet gastritis kronik ranitidine 150 mg safe. The clinician must be succesful of interpret these checks singly and in combination depending on the etiology of the liver disease and the scientific inquiries to be requested. Future research will concentrate on understanding the best purposes of noninvasive testing for prediction of medical outcomes and responses to treatment. Bedossa P: Intraobserver and interobserver variations in liver biopsy interpretation in sufferers with continual hepatitis C. Foster G, et al: Management of continual hepatitis C: medical audit of biopsy primarily based administration algorithm. Angulo P, et al: Liver fibrosis, however no different histologic options, associates with long-term outcomes of patients with nonalcoholic fatty liver disease. Poynard T, et al: Staging chronic hepatitis B into seven classes, defining inactive carriers and assessing therapy impression utilizing a fibrosis biomarker (FibroTest) and elastography (FibroScan). Kamimoto Y, et al: Plasma clearance of intravenously injected aspartate aminotransferase isozymes: evidence for preferential uptake by sinusoidal liver cells. Sud A, et al: Improved prediction of fibrosis in persistent hepatitis C using measures of insulin resistance in a chance index. Imbert-Bismut F, et al: Biochemical markers of liver fibrosis in patients with hepatitis C virus infection: a prospective examine. Suzuki A, et al: Hyaluronic acid, an accurate serum marker for severe hepatic fibrosis in sufferers with non-alcoholic fatty liver disease. Tamaki S, et al: Evaluation of hyaluronic acid binding capacity of hepatic sinusoidal endothelial cells in rats with liver cirrhosis. Li J, et al: Tissue inhibitor of metalloproteinase is elevated within the serum of precirrhotic and cirrhotic alcoholic sufferers and might serve as a marker of fibrosis. Patel K, et al: Evaluation of a panel of non-invasive serum markers to differentiate gentle from moderate-to-advanced liver fibrosis in persistent hepatitis C sufferers. Rosenberg W, et al: Serum markers detect the presence of liver fibrosis: a cohort study. Allan R, Thoirs K, Phillips M: Accuracy of ultrasound to establish persistent liver illness. Di Lelio A, et al: Cirrhosis: diagnosis with sonographic examine of the liver floor. Simonovsk� V: the analysis of cirrhosis by excessive resolution ultrasound of the liver surface. Schneider A, et al: Noninvasive evaluation of liver steatosis, fibrosis and inflammation in continual hepatitis C virus an infection. Saadeh S, et al: the utility of radiological imaging in nonalcoholic fatty liver illness. Stark D, et al: Magnetic resonance imaging and spectroscopy of hepatic iron overload. Lebray P, et al: Liver stiffness is an unreliable marker of liver fibrosis in sufferers with cardiac insufficiency. Arena U, et al: Liver stiffness is influenced by a standardized meal in patients with persistent hepatitis C virus at completely different levels of fibrotic evolution. Huwart L, et al: Magnetic resonance elastography for the noninvasive staging of liver fibrosis. Nightingale K, et al: Acoustic radiation pressure impulse imaging: in vivo demonstration of clinical feasibility. Friedrich-Rust M, et al: Liver fibrosis in viral hepatitis: noninvasive assessment with acoustic radiation pressure impulse imaging versus transient elastography 1. Chen S-H, et al: Effects of affected person components on noninvasive liver stiffness measurement utilizing acoustic radiation pressure impulse elastography in patients with persistent hepatitis C. American Association for the Study of Liver Diseases, Infectious Diseases Society of America: Recommendations for testing, managing, and treating hepatitis C, 2014. Poynard T, et al: Meta-analyses of FibroTest diagnostic value in persistent liver illness. Leroy V, et al: Prospective evaluation of FibroTest, FibroMeter, and HepaScore for staging liver fibrosis in persistent hepatitis B: comparability with hepatitis C. Guo Y, et al: Magnetic resonance elastography and acoustic radiation drive impulse for staging hepatic fibrosis: a meta-analysis. Friedrich-Rust M, et al: Performance of acoustic radiation drive impulse imaging for the staging of liver fibrosis: a pooled metaanalysis. Cast�ra L, et al: Prospective comparison of two algorithms combining non-invasive methods for staging liver fibrosis in persistent hepatitis C. Vergniol J, et al: the evolution of non-invasive tests of liver fibrosis is associated with prognosis in patients with continual hepatitis C. Kim S, et al: Factors that have an effect on the diagnostic accuracy of liver fibrosis measurement by Fibroscan in patients with persistent hepatitis B. Li J, et al: the validity of serum markers for fibrosis staging in persistent hepatitis B and C. Marcellin P, et al: Non-invasive evaluation of liver fibrosis by stiffness measurement in sufferers with continual hepatitis B. Fung J, et al: Correlation of liver stiffness and histological features in wholesome individuals and in patients with occult hepatitis B, persistent energetic hepatitis B, or hepatitis B cirrhosis. Oliveri F, et al: Liver stiffness in the hepatitis B virus carrier: a non-invasive marker of liver disease influenced by the pattern of transaminases. Vigan� M, et al: Transient elastography evaluation of the liver stiffness dynamics during acute hepatitis B. Bedogni G, et al: Prevalence of and risk components for nonalcoholic fatty liver illness: the Dionysos nutrition and liver study. Chalasani N, et al: the diagnosis and administration of non-alcoholic fatty liver disease: apply guideline by the American Association for the Study of Liver Diseases, American College of Gastroenterology, and the American Gastroenterological Association. Festi D, et al: Review article: the analysis of non-alcoholic fatty liver disease-availability and accuracy of non-invasive strategies. Gaia S, et al: Reliability of transient elastography for the detection of fibrosis in non-alcoholic fatty liver disease and chronic viral hepatitis. Petta S, et al: Reliability of liver stiffness measurement in nonalcoholic fatty liver disease: the results of physique mass index. Petta S, et al: the severity of steatosis influences liver stiffness measurement in sufferers with nonalcoholic fatty liver illness. Sasso M, et al: Novel controlled attenuation parameter for noninvasive assessment of steatosis utilizing Fibroscan: validation in continual hepatitis C. Cui J, et al: Comparative diagnostic accuracy of magnetic resonance elastography vs. Angulo P, et al: Simple noninvasive methods predict long-term outcomes of patients with nonalcoholic fatty liver illness.
Discount ranitidine 150 mg onlineMany totally different illnesses are characterised by pigmentary retinopathy diet in gastritis ranitidine 300 mg discount mastercard, and the presentation gastritis diet 500 ranitidine 150 mg cheap online, progression, and extent of visual loss differ extensively. Patients have iris transillumination defects by which the purple reflex is seen through multiple punctate defects in the iris. Absence of pigment within the retinal pigment epithelium layer of the retina makes the fundus seem a lighter yellowish-orange color than ordinary. The choroidal vasculature, usually hidden by the retinal pigment epithelium, is seen. The macula and fovea are variably hypoplastic, and visual acuity relies on the level of pigment current and on the event of the macula and fovea. Such sufferers have iris transillumination defects, fundus hypopigmentation, and photophobia. Peripheral telangiectasia along the course of the retinal vasculature results in exudation, giving the retina a yellowish-white look. In kids, pigmentary modifications may not be as superior or as noticeable as in adults. The retinal pigment epithelial changes embrace deposition of pigment in a perivascular sample. Patients with sensorineural listening to loss ought to be examined for the associated presence of retinitis pigmentosa (Usher syndrome and Hallgren syndrome). Renal illness together with Fanconi syndrome, cystinuria, cystinosis, and oxalosis could additionally be related to pigmentary retinal changes, as could the mucopolysaccharidoses, Refsum illness, and syphilis. Retinal Detachment Trauma is the most common explanation for retinal detachment in kids. Large retinal detachments may produce loss of the purple reflex, and leukocoria happens when the detached retina is in apposition to the lens or when vital scarring (proliferative vitreoretinopathy) is present. Symptoms of retinal detachment embrace photopsias (flashing lights); floaters (caused by vitreous hemorrhage); and changes in imaginative and prescient, together with blurring of imaginative and prescient or the sensation of a veil or curtain blocking imaginative and prescient. Mild forms have an effect on the peripheral retina at the junction between the vascularized and immature avascular retina. These modifications could be noticed solely with an indirect ophthalmoscope and scleral depression. A white fibrovascular mass may occupy the retrolental area (retrolental fibroplasia) and produce leukocoria. The inferior retina is detached, and a demarcation line between the connected and detached retina is seen. Fluid beneath the indifferent sensory retina shifts with movement of the eye and causes the indifferent retina to move or undulate with movement of the attention. Retinitis and Retinochoroiditis Inflammation of the retina and choroid is mostly the result of viral, protozoal, fungal, or bacterial an infection. The last frequent pathway for restoration or resolution of retinal inflammation is the manufacturing of a pigmented chorioretinal scar. The characteristics and placement of these scars are regularly, but not at all times, suggestive of a analysis. Sympathetic ophthalmia occurs after a extreme harm involving the uvea of one eye, the "thrilling" eye, adopted by a latent period and the development of uveitis in the uninjured eye, the "sympathizing" eye. Sympathetic ophthalmia may happen as early as 10 days after the original harm but can also have a delayed onset years after the incident. Sympathetic ophthalmia is an autoimmune disorder, and therapy is with topical and systemic immunosuppression. Acute, recurrent, chorioretinal irritation might happen adjacent to pigmented scars. Infants congenitally contaminated may have widespread involvement resulting in fetal demise if maternal infection happens within the first or early within the second trimester. If an infection happens within the third trimester, results could include chorioretinitis and encephalomyelitis, however the being pregnant will likely be viable. Congenital illness can also occur in inactive and recurrent forms, the effects of which can be restricted to retinitis alone. Toxoplasmosis may be acquired, with an infection being widespread with increasing age. The retinal lesions are regularly asymptomatic and are found incidentally as inactive pigmented chorioretinal scars. Inactive lesions could reactivate at any time throughout life, with energetic irritation growing adjacent to areas of scarring. Patients with lesions close to the macula or optic nerve ought to be wary of any visual adjustments. Patients too younger to report visible modifications must be screened periodically for reactivation of their disease. Rubella Exposure to rubella virus during the first trimester of pregnancy results in an intrauterine an infection manifested as congenital rubella syndrome. Ocular findings embrace microphthalmia, microcornea, corneal opacification, anterior uveitis, iris hypoplasia, nuclear or complete cataracts, and glaucoma. Retinitis, with hemorrhages and perivascular yellowish-white exudates secondary to cytomegalic inclusion disease. Other ophthalmic manifestations embrace microphthalmia, uveitis, cataracts, optic disc atrophy, strabismus, and nystagmus. Retinal inflammation, edema, and hemorrhage could additionally be in depth and quickly progressive in these sufferers. Herpes Simplex Virus Herpes simplex virus an infection might contain the anterior segment of the eye, with conjunctivitis, keratitis, and iritis or, particularly when disseminated in the perinatal period, a retinochoroiditis might develop. Retinal involvement with disseminated herpes simplex virus is severe, with intensive inflammatory reaction producing yellowish-white exudates and retinal necrosis. Herpetic retinitis may happen in regular individuals however is more common in the immunosuppressed. Syphilis Congenital syphilis might cause bilateral chorioretinitis, resulting in a salt-and-pepper fundus appearance. Differentiation of the retinopathy of congenital syphilis from retinitis pigmentosa could also be tough. Syphilis may trigger interstitial keratitis, anterior uveitis, glaucoma, and optic nerve atrophy. Toxocariasis Toxocara canis larvae infect children mostly from 2 to 9 years old. Chronic unilateral uveitis with opacification of the vitreous overlying the granuloma may happen. Inflammation in ocular toxocariasis occurs only after the infecting organism dies. With extensive irritation, fibrotic preretinal membranes may develop and produce retinal detachment. There are small flame-shaped hemorrhages within the nerve fiber layer that follow the pattern of the retinal vessels. More intensive areas of hemorrhage have broken by way of to the preretinal house and are seen as areas of blood that obscure the retina. Dragonwort (Bistort). Ranitidine.
Source: http://www.rxlist.com/script/main/art.asp?articlekey=96120
Ranitidine 150 mg cheap otcAlthough both diagnoses comprise a phase on the continuum of disease and inflammation gastritis lemon discount 300 mg ranitidine otc, therapy implications range gastritis diet ýðîòèêà purchase ranitidine 150 mg visa. This process requires proper equipment, together with a pneumatic otoscope head and an appropriately sized speculum to obtain an excellent air seal. When a seal is troublesome to acquire despite proper speculum measurement, the head and tubing should be checked for air leaks. If none is discovered, utility of a piece of rubber tubing to the tip of the speculum (shown attached to the otoscope) or use of a gentle speculum (1) might solve the issue. The bulb is then gently and slowly pressed and launched whereas the mobility of the drum is assessed. Pressing on the bulb applies constructive strain; letting up applies unfavorable strain. C, In instances of acute otitis media, in which the center ear is full of purulent materials, the drum bulges toward the examiner and strikes minimally. D, In instances of acute otitis media with an air/fluid level, mobility could also be practically regular. In some sufferers, nonetheless, the drum could also be retracted, indicating elevated adverse pressure. If that is the case, mobility on optimistic strain could additionally be lowered, whereas motion on adverse stress is type of normal or only mildly decreased. E, this is identical pattern as that seen commonly in youngsters with continual serous otitis. F, In cases of high unfavorable pressure and no effusion, application of constructive stress produces little or no motion, however on negative pressure the drum billows again toward the examiner. The prognosis may also be made with delicate bulging and up to date symptoms or redness of the tympanic membrane. Although this phenomenon is mostly related to Mycoplasma an infection in adults, any of the standard pediatric pathogens (see Table 24. Finally, acute otitis media might, by advantage of increasing center ear strain, result in acute perforation of the tympanic membrane. A, this is the textbook picture-an erythematous, opaque, bulging tympanic membrane. B, In this acutely febrile baby who complained of otalgia, the presence of both air and fluid fashioned bubbles separated by grayish-yellow menisci. Even though the drum was not injected, this discovering, combined with fever and otalgia, is consistent with acute infection. C, In this child, the tympanic membrane was injected on the periphery, and a yellow purulent effusion triggered the inferior portion to bulge outward. Although some sufferers have extreme otalgia, others may complain of sore throat, gentle ear discomfort, ear popping, or decreased hearing but have floridly infected eardrums. Radiographic research are usually of little worth within the analysis of acute otitis media. Treatment for acute otitis media could embrace the choice of remark with out use of antibiotics based on age, illness severity, and assurance of follow-up. In addition to treating patients with an appropriate antimicrobial agent and analgesics when essential, follow-up examination is necessary. This is finest carried out 2 to 3 weeks after analysis, when complete resolution can be anticipated in additional than 50% of kids. Selected older patients with gentle, uncomplicated acute otitis media could additionally be observed with out antimicrobial remedy, however follow-up examination is still essential. Children with recurrent episodes of otitis media are candidates for tympanostomy tubes. Guideline numbers of infections are three episodes in 6 months or 4 episodes in 1 year with one episode within the preceding 6 months. Otitis Media With Effusion (Serous Otitis Media) Serous effusion in the center ear could end result from an higher respiratory tract infection, or it might be the residual of treated acute otitis. Persistence appears to lead to part from eustachian tube dysfunction with poor drainage and air flow. Pneumatic otoscopy usually reveals poor mobility of the tympanic membrane, and mobility is noted totally on unfavorable pressure. The latter is thought to develop on account of absorption of center ear gases by mucosal cells, creating a vacuum that persists with the fluid due to failure of air flow by the eustachian tube. Chronic Otitis Media With Effusion Chronic otitis media with effusion is widespread in younger youngsters. Patients subject to this situation seem to have important and prolonged eustachian tube dysfunction. On otoscopy, an erythematous bullous lesion is seen obscuring much of the tympanic membrane. This phenomenon, referred to as bullous myringitis, is attributable to the usual pathogens of otitis media in childhood. The bullous lesion often ruptures and drains spontaneously, providing quick aid of pain. In this youngster, increased middle ear pressure with acute otitis resulted in perforation of the tympanic membrane. Less commonly, immunodeficiency and immotile cilia syndrome are identified as underlying etiologic conditions. Chronic otitis media is associated with vital morbidity when it comes to intermittent or persistent listening to impairment, intermittent discomfort, and the sequelae of recurrent an infection. Persistence of a serous effusion for longer than three to four months with important hearing loss is also a sign for myringotomy and insertion of tubes. The tube serves to vent the center ear, enhance hearing, and scale back the frequency of infection. There are many different types in a wide range of shapes, materials, sizes, and colours. It can present as a defect within the tympanic membrane through which persistent drainage happens, or it can appear as a white cystic mass behind or involving the eardrum. B and C, Acquired cholesteatomas, which generally current after an extended history of chronic middle ear disease. Although a number of are congenital with an intact tympanic membrane, the majority are sequelae of untreated or chronic/recurrent otitis media with a tympanic membrane defect. The commonest explanation for aural polyps in youngsters is an old, retained tympanostomy tube. These tissues typically bleed simply, which might frighten the patient, the mother or father, and the physician. A, Growth of this polypoid granuloma was stimulated by the inflammatory process of continual middle ear infection. B, these polyps, which protrude through a tympanic membrane perforation, have enlarged to totally fill the external ear canal. 300 mg ranitidine generic with amexC gastritis and constipation discount 300 mg ranitidine with mastercard, A 21-year-old man with severe respiratory involvement and an unsuspected proper pneumothorax gastritis yeast infection cheap ranitidine 150 mg free shipping. In sweat testing, pilocarpine is pushed into the skin with a weak electrical current (iontophoresis), and the ensuing sweat is collected with a wristband containing a coiled capillary tube, which wicks the sweat and stores it for evaluation. The sweat check should be performed in an skilled laboratory, similar to these related to one of the Cystic Fibrosis Foundation�approved cystic fibrosis facilities. Both false-negative and false-positive outcomes are alarmingly common in inexperienced hands. Sweat chloride values of 40 to 60 mEq/L (or 30 to 60 mEq/L in infants <6 months old) are thought of borderline and usually require a second take a look at. False-positive values can occasionally occur, but problems that trigger this are readily distinguished clinically from cystic fibrosis. Other entities that will elevate sweat chloride include adrenal insufficiency, ectodermal dysplasia, nephrogenic diabetes insipidus, hypothyroidism, mucopolysaccharidoses, glucose-6-phosphatase deficiency, hypoproteinemia, malnutrition, and exposure to topiramate. Patients with cystic fibrosis who present with extreme malnutrition and edema may have false-negative values on preliminary sweat exams until their dietary status improves. Genetic testing is type of useful in the evaluation of the toddler who produces too little sweat for analysis, the patient with borderline sweat chloride, or the affected person with regular sweat chloride however clinical options attribute of cystic fibrosis. Mutation-specific therapies have been proposed in cystic fibrosis, and due to this fact genetic testing of all patients with cystic fibrosis is recommended. Thickened airways are seen in longitudinal part through the upper lobes (A) and in cross-section in a picture from the lower lobes (B). Counseling dad and mom to smoke outside the house and automobile is one other important intervention that pediatricians could make. These events are often related to forceful respiratory efforts and a color change. Studies also embrace a sleep examine that measures respiratory and stomach wall movement, airflow on the mouth or nose, pulse oximetry and heart fee and, in some instances, pH monitoring of the distal esophagus. The latter group contains patients with Crouzon syndrome, Apert syndrome, Down syndrome, Treacher Collins syndrome, the Pierre Robin sequence, ArnoldChiari malformation, Prader-Willi, M�bius syndrome, and dwarfism. The arousal-plusawakening index can quantify the severity of the consequences of sleepdisordered respiration on the standard of sleep and help direct administration. Mixed apnea occurs when an obstructive apneic episode is followed by a central pattern of apnea (or vice versa). The generally used phrases to describe these forms are "aspiration from above" and "aspiration from beneath. Ongoing aspiration of saliva results in a progressive injury to the lung and worsening respiratory impairment. It is persistent aspiration that leads to the untimely dying that happens in most children with profound neurologic impairment. Microaspiration, which refers to aspiration of tiny, essentially undetectable quantities of gastric contents, may cause intense bronchospasm as a result of the acidity of the aspirated materials. Absence of airflow accompanied by the cessation of chest and abdominal wall motion distinguishes central apnea. Obstructive apnea is the most typical form of apnea and is characterized by the lack of airflow on the nose or mouth regardless of continued respiratory efforts. Chest radiograph of a 20-year-old with lifelong continual, severe aspiration exhibits elevated interstitial markings and areas of consolidation-atelectasis. Aspiration ought to be suspected in sufferers with poorly managed bronchial asthma regardless of aggressive management of asthma, especially in sufferers with neurologic impairment. Parameters assessed in the course of the modified barium swallow embrace the entire following: initiation of the swallow (timing and oral control); period of the swallow; adequacy of the swallow to clear food bolus; presence, quantity, and timing of aspiration; protective reactions in response to aspiration; and taste bud management throughout swallowing. In neurologically-impaired individuals, particularly those fed by way of feeding tubes, the radionuclide "salivagram" is a fast technique of figuring out whether or not the affected person is aspirating his or her oral secretions. A small radioactive bolus is positioned underneath the tongue, and the affected person is then monitored under a gamma digital camera. It leads to a low radiation dose to the patient, similar to that of the chest radiogram and a fraction of that utilized in a barium swallow. The radionuclide gastric emptying or "milk" scan, which makes use of the identical radiation dose because the salivagram, can show reflux and delay in gastric emptying. Globules of fats present in a predominance of the macrophages recommend aspiration of meals. If seen in average and excessive numbers, this discovering is particular for aspiration of food, either the result of irregular swallowing or from refluxed gastric contents. Interpretation of pulmonary operate take a look at leads to youngsters must take into account variability in performance by children and differences in age, peak, weight, intercourse, and race. In youngsters, pulmonary operate exams may be helpful in establishing the severity of respiratory illness, in guiding the choice of therapy, and in measuring the response to a therapeutic regimen. In some illnesses, corresponding to cystic fibrosis or asthma, proof of increasing airway obstruction might indicate the want to provoke or improve the aggressiveness of therapeutic intervention. The preliminary portion of the flow-volume curve is effort dependent, whereas the terminal 25% of the expiratory maneuver depends on elastic recoil and airway resistance and is comparatively impartial of patient effort. With elevated airway resistance distal to the central, large airways, the curve turns into concave toward the abscissa (volume axis). Spirometry can additionally be used to document reversibility of obstruction after bronchodilator inhalation. Patients with suspected asthma may develop this configuration of flow-volume curve after bronchoprovocation exams, similar to inhaled histamine, methacholine, chilly air, or after exercise testing. Fixed obstruction of the upper airways, similar to in tracheal stenosis, produces a limitation and plateau of each the inspiratory and expiratory loops of the flow-volume curve. A reduced inspiratory flow and a plateau of the inspiratory loop are suggestive of variable extrathoracic obstruction seen in disorders corresponding to laryngomalacia and vocal cord dysfunction. Disease states that have an effect on lung progress can be expected to alter lung quantity along with airway caliber. These illnesses embrace pulmonary hypoplasia due to extreme oligohydramnios or area occupying lesions. A, Fixed airway obstruction with reduction in inspiratory and expiratory move charges. B, Variable extrathoracic airway obstruction, with lowered peak inspiratory flow charges. The subject makes small panting maneuvers, leading to small changes in the volume of the lung and corresponding inverse volume adjustments in the box. This permits for calculation of the lung volume at which the panting efforts began. Although an increased residual quantity to total lung capability ratio is often a hallmark of obstructive lung disease, this may also be exhibited in patients with neuromuscular weak spot. In a cooperative affected person, this can be correlated with examination or respiratory muscle energy (maximum inspiratory and expiratory pressure measurements).
Generic ranitidine 300 mg lineAlthough care should be taken during the procedure to prevent brachial plexus harm gastritis symptoms toddler buy cheap ranitidine 150 mg online, surgical procedure carried out before adolescence usually improves appearance and restores some function diet when having gastritis safe ranitidine 300 mg. It is assumed to end result from a failure of maturation of the ossification middle of the clavicle. It typically involves the proper aspect and every so often may be associated with other congenital anomalies and could be seen in patients with neurofibromatosis 1. In cleidocranial dysostosis, the entire clavicle could also be absent or may have an appearance just like that of congenital pseudarthrosis. This situation characteristically includes no practical impairment and requires no therapy. Radial Club Hand Radial membership hand is the results of congenital absence or hypoplasia of the radial buildings of the forearm and hand. A, the forearm is shortened with radial deviation of the hand and wrist on the ulna. B, A flexion deformity of the hand and wrist on the forearm and a hypoplastic thumb are current. C, Radiograph exhibits absence of the radius, dislocation of the carpus, and a rudimentary thumb, all characteristic of radial club hand. Treatment is best instituted early with passive stretching workouts and corrective casting. Surgical therapy consists of centralization of the hand on the "one-bone forearm" to maximize perform. Ganglion of the Wrist A ganglion is a benign cystic mass consisting of an accumulation of synovial fluid or gelatin in an outpouching of a tendon sheath or joint capsule. On examination, they may be either firm or fluctuant, and they can be transilluminated. Although most are asymptomatic, an occasional patient could complain of ache and tenderness. Surgical excision with obliteration of the bottom of the ganglion is the most profitable remedy for the occasional patient in whom treatment is indicated. It could additionally be related to different congenital anomalies, notably Apert syndrome and Streeter dysplasia. In more severe circumstances, the nails, deeper constructions, and bones could additionally be conjoined, contributing to deformity and growth abnormalities and making reconstructive treatment more difficult. Syndactyly Syndactyly is a comparatively common congenital anomaly involving failure of the digits of the arms or toes to separate. This cystic mass overlying the wrist joint and flexor tendons was asymptomatic and nontender. This is the outcome of an unrecognized or inadequately handled damage to the extensor tendon at its insertion on the middle phalanx. This youngster has delicate syndactyly involving gentle tissues of the middle and ring fingers without bony involvement. It is assumed to outcome from tightness of the tendon sheath of the flexor pollicis longus within the region of the metacarpophalangeal joint. If passively correctable, splinting in extension often results in correction; otherwise, surgical procedure is required. A boutonni�re deformity of a finger is the tip result of a traumatic avulsion of the central portion of the extensor tendon at its insertion on the middle phalanx that went unrecognized on the time of initial harm. Mallet Finger/Swan-Neck Deformity A mallet finger is the outcomes of avulsion of the extensor tendon from its insertion on the base of the distal phalanx of a finger. The tendon alone, or a portion of the distal phalanx into which it inserts, could also be involved. There is a hard and fast flexion deformity on the interphalangeal joint of the thumb resulting from tightness of the tendon sheath of the flexor pollicis longus. This is the outcomes of avulsion of the extensor tendon from its insertion on the base of the distal phalanx, which was not acknowledged on the time of harm. A disability ensuing from a deformed, shortened, or painful lower limb may be considerable (see the Gait and Gait Disturbances part, earlier). Many problems of the lower extremities occurring in childhood are congenital and may end up in lifelong disability if they proceed to be unrecognized or are unsuccessfully treated. Knowledge of the traditional anatomy and function of the hip, knee, ankle, and foot is necessary to accurately acknowledge and treat abnormalities on this region (see the Lower Extremity Examination part, earlier). Developmental Dislocation of the Hip Developmental dislocation of the hip, previously referred to as congenital dislocation of the hip, consists of displacement of the femoral head from its regular relationship with the acetabulum. Female infants are affected significantly extra regularly than male infants, and unilateral dislocation is twice as frequent as bilateral. Idiopathic dislocation is more frequent, and sufferers usually have a optimistic family historical past for the defect. Its severity varies from subluxated, to dislocated and reducible, to dislocated and irreducible. This type of developmental dislocation could also be associated to abnormal intrauterine positioning or restriction of fetal motion in utero, which impedes adequate development and stability of the hip joint complex. The relaxing impact of hormones on soft tissue during pregnancy may contribute, with affected infants maybe being more sensitive to the pelvic leisure effects of maternal estrogen. Teratogenic dislocations of the hip represent a extra severe form of the disorder and are in all probability the result of a germ plasm defect. They occur early in fetal improvement and result in malformation of both the femoral head and the acetabular socket. Associated congenital anomalies are common in infants whose dislocations are teratogenic, including clubfoot deformity, congenital torticollis, metatarsus adductus, and infantile scoliosis. Early analysis allows prompt institution of remedy and ends in a better outcome. Knowledge of the medical signs and ability in strategies of examination are needed. Typically, the toddler with a dislocated hip has no noticeable difference within the place in which the leg is held, though some affected infants could maintain the leg ready of adduction and exterior rotation. This foreshortening is accentuated by holding the hips and knees in 90 degrees of flexion (Galeazzi sign). In sufferers with reducible dislocations, the Ortolani signal is positive when a palpable clunk is felt on abduction and inner rotation (relocation) of the hip. The Barlow take a look at is optimistic if, with the knees flexed and hips flexed to 90 levels, the hips are gently adducted with pressure applied on the lesser trochanter by the thumb. A palpable clunk indicating posterior dislocation is appreciated if the hip is unstable or dislocated. When the hip is dislocated and irreducible, solely limitation of abduction is apparent. Furthermore, in developmental dislocation, ossification may be delayed even longer, because regular articulation forces are absent.
300 mg ranitidine generic free shippingA history of antecedent upper respiratory tract or pores and skin infection is current in over 50% of cases gastritis or appendicitis purchase 150 mg ranitidine with visa. Systemic symptoms consist primarily of fever and irritability in association with refusal to stroll gastritis diet ãîðîñêîï 300 mg ranitidine cheap with visa, limp, or decreased use of an extremity. A small percentage present with more severe systemic symptoms, together with chills, lethargy, irritability, anorexia, vomiting, and dehydration. At this age, kids are sometimes unable to localize ache, however by statement they could be found to avoid shifting the concerned extremity or to hold a specific joint in flexion persistently. Soft tissue swelling and warmth may be noted overlying a metaphysis, however it may be delicate or absent in early circumstances or undetectable if the proximal femur is concerned. Even with careful examination, focal tenderness may be difficult to detect early within the course. Children older than 2 years old with acute osteomyelitis are sometimes febrile however hardly ever toxic. They usually tend to localize ache, and point tenderness is usually simple to elicit. Unless sympathetic effusion has developed, the adjoining joint could additionally be passively moved through its full vary of motion, though this exacerbates the pain. Osteomyelitis in sites aside from the lengthy bones of the extremities can be difficult. Although fever and an abnormal gait are the most common presenting complaints, decrease belly and groin ache, hip or buttock pain, sciatica, and thigh ache (with swelling) could be distinguished early complaints. Often, the initial medical image suggests appendicitis, pelvic abscess, or femoral osteomyelitis. A excessive level of suspicion and cautious examination are necessary to establish the analysis. The onset of ache within the lower abdomen somewhat than the periumbilical area, absence of gastrointestinal signs or rebound tenderness, and normal findings on rectal examination assist distinguish pelvic osteomyelitis from acute appendicitis. Furthermore, though most sufferers have ache on hip motion in one or more planes, vary of motion is either regular or only slightly restricted, and with cautious examination, point tenderness can often be detected. Acute Osteomyelitis Due to Contiguous Spread Acute osteomyelitis resulting from the contiguous spread of infection should be suspected in patients with prior puncture wounds, deep lacerations, surgical incisions or hardware, open fractures, abscesses, or cellulitis who expertise a sudden onset of elevated pain on the web site. This pain is perceived as deep, severe, and constant and is aggravated by motion. Osteomyelitis because of extension of major delicate tissue an infection may current as worsening after a interval of preliminary enchancment or failure to response to antimicrobials. Diagnostic Methods in Acute Osteomyelitis Standard laboratory and radiographic studies are of limited use within the analysis of acute osteomyelitis. These markers are helpful in identifying an inflammatory course of and for serial measurement to document response to remedy. Plain radiographic changes lag behind the medical manifestations and could be refined. Subsequently, the swelling will increase, obliterating fascial planes, and extends to involve subcutaneous tissues. These gentle tissue modifications may be tough to appreciate each time osteomyelitis involves vertebrae or pelvis; nevertheless, in cases of pelvic osteomyelitis, clouding of the obturator foramen, distortion of the fascial planes around the adjoining hip, or even displacement of the bladder could additionally be detectable. Technetium scans are also useful in delineating further foci within the rare patients with multiple websites. Standard radiographs stay essential in identifying fractures and malignancies, which can simulate the looks of osteomyelitis on bone scans. Importantly, 5% to 20% of children with acute osteomyelitis can have a false-negative bone scan in the course of the first few days. Fever, hip and thigh pain, and refusal to walk had been the chief complaints in this 5-year-old youngster with osteomyelitis of the proximal femur. On inspection, she lay nonetheless, holding the left leg externally rotated and flexed at the hip and knee. A, the primary noticeable change, occurring about 3 days after onset, is deep gentle tissue swelling, seen right here adjoining to the metaphysis of the distal tibia on the left. B, In this neonate, a radiolucency is obvious in the proximal metaphysis of the proper femur, which can be displaced upward and laterally. On aspiration of the hip, purulent fluid was obtained, confirming the suspicion of rupture of the infection into the hip and of secondary septic arthritis. C, this 1-year-old female presented with 4 days of fever and lack of proper arm use. E, the late changes of a lytic lesion with sclerotic margins are seen in the proper femoral metaphysis of this child who was finishing his course of therapy. Vigorous makes an attempt are important to isolate the causative organism and determine antimicrobial susceptibilities, significantly within the era of increasing antibiotic resistance. Aspiration of the location of maximal involvement as revealed by imaging supplies material for Gram stain and culture. Blood cultures are optimistic in more than 50% of sufferers with acute hematogenous osteomyelitis and should be performed in all suspected cases. Complications of osteomyelitis embrace secondary septic arthritis with resultant joint damage, epiphyseal damage with long-term morbidity ensuing from impaired bone development, progression to persistent osteomyelitis (now fewer than 4% of cases), and infrequently pathologic fractures. The price of issues is highest in younger infants who typically have intensive bone involvement and secondary septic arthritis by the point the analysis is made. Care in clinical assessment and aggressive makes an attempt to verify the prognosis as early as possible are important, as are adequate antimicrobial remedy and surgical intervention. Subacute Osteomyelitis Approximately 10% of circumstances of hematogenous osteomyelitis have an insidious onset and a subacute course characterized by mild to moderate native extremity pain, with or without swelling. In some cases, this subacute course may be associated to partial suppression of the an infection by antibiotics administered for one more infection (such as, otitis media or impetigo). In these sufferers, pain could abate throughout antimicrobial therapy but worsen once the medicine stops. On examination, native tenderness is clear and overlying gentle tissue swelling could also be famous. Biopsy is usually required to affirm the analysis and isolate the causative organism. A and B, this 13-year-old boy had a 7-week history of pain and swelling of both ankles. These radiographs show bilateral gentle tissue swelling, a number of metaphyseal radiolucencies in the distal left tibia, and a radiolucency involving the metaphysis and epiphysis on the right. C, An extensive area of radiolucency and cortical response is seen in the ulnar diaphysis of this teenager. D, Obliterated fascial planes, radiolucency and periosteal new bone formation is seen. Chronic Osteomyelitis With antimicrobial therapy and improved diagnostic strategies, persistent osteomyelitis has turn into a lot less common in developed nations. Delay in prognosis, inadequate antimicrobial or surgical remedy, and resistant organisms are the major elements now associated with persistent disease.
Cheap 150 mg ranitidine amexA gastritis green tea ranitidine 300 mg amex, Planar bone scan demonstrates focal activity within the fifth lumbar vertebra of the backbone gastritis symptoms months ranitidine 300 mg discount on line. These scans are useful for preliminary staging, for assessment of therapy response, for disease monitoring after completion of therapy, to differentiate residual tumor from a scar or necrosis, and to assess prognosis. Reference Pruckmayer M, Zacherl S, Salzer-Muhar U, et al: Scintigraphic evaluation of pulmonary and whole-body blood circulate patterns after surgical intervention in congenital coronary heart disease, J Nucl Med forty:1477�1483, 1999. In the method, the liver generates enough metabolic warmth to be a major source of core homeostatic temperature upkeep. Gross Anatomy the mature liver lies primarily in the right hypochondriac and epigastric areas of the abdominal cavity, beneath the diaphragm. In adults, the wholesome liver weighs approximately 1400 g to 1600 g and extends along the midclavicular line from the best fifth intercostal area to simply inferior to the costal margin. The anterior border of the liver then extends medially and crosses the midline simply inferior to the xiphoid process. A small portion of the organ projects across the midline and lies within the upper left stomach quadrant. The liver is incompletely separated into lobes which are covered on their exterior surfaces by a thin connective tissue capsule. The proper lobe is further subdivided inferiorly and posteriorly into two smaller lobes-the caudate and quadrate lobes. First is a plane that passes by way of the gallbladder and inferior vena cava, to the best of the midplane of the abdomen, that defines the halves of the liver supplied by the right and left branches of the portal vein and hepatic artery, along with biliary drainage into the proper and left hepatic ducts. As a outcome, the quadrate lobe and a big portion of the caudate lobe are located to the best of the groove of the inferior vena cava but belong functionally to the left hemiliver. Further functional subdivision of the liver into eight segments having impartial vascular and biliary supplies enables surgeons to resect segments of the liver whereas maintaining relative hemostasis. On the convex liver surface dealing with the stomach cavity this connective tissue layer is covered by the simple squamous mesothelial cells of the peritoneal serosal lining. At the superior site of attachment of the Introduction the liver is the largest organ within the human physique. The proper and left leaves of the falciform ligament then merge with reflections of the parietal peritoneum extending from the diaphragm forming, respectively, the triangular ligament over the left dome of the liver and the coronary ligament over the best dome of the liver. The posterior side of the liver is covered by peritoneal serosa, with reflections on the groove of the inferior vena cava into which the a quantity of hepatic veins empty. The dual blood provide of the liver enters the organ at its hilus (porta hepatis) accompanied by the hepatic bile duct, lymphatics, and nerves. Approximately 80% of the blood coming into the liver is poorly oxygenated and is supplied by the portal vein. The remaining 20% of the hepatic blood provide is well oxygenated and delivered by the hepatic artery. Briefly, the liver primordium seems in human embryos through the third week of gestation as an endodermal bud from the ventral foregut simply cranial to the yolk sac. This bud turns into the hepatic diverticulum as it enlarges, elongates in a cranio-ventral fashion, and develops a cavity contiguous with the foregut. The hepatic diverticulum consists of three portions: (1) the hepatic portion varieties the hepatic corpus, including parenchymal cells and the weather of the portal tree; (2) the cystic portion types the gallbladder; and (3) probably the most ventral portion forms the head of the pancreas. The hepatic portion grows into the septum transversum-a plate of mesenchyme that incompletely separates the thoracic and peritoneal cavities. During the fourth week of growth, buds of epithelial cells prolong from the hepatic diverticulum into the mesenchyme of the septum transversum as thick multicellular anastomosing cords. They turn into interspersed within the growing anastomotic network of capillaries arising from the symmetrically arranged vitelline veins returning from the stomach cavity of the embryo, thus starting to establish the shut relationship of the hepatic parenchymal cells to the sinusoids. Blood draining from the parenchymal sinusoidal plexus throughout the nascent liver passes through the symmetric proper and left hepatocardiac channels, to enter the sinus venosus. This embryonic vascular pattern provides method to the definitive fetal vascular sample by the seventh week: the paired vitelline veins unite to type a single portal vein, which divides into proper and left branches upon getting into the liver, and arterial sprouts from the hepatic arterial branch of the celiac axis course along the intrahepatic portal tree and turn out to be the organizing elements for formation of the intrahepatic biliary tree. Between the sixth week and birth the fetal liver serves as a hematopoietic organ and as the main website for fetal blood formation until the third trimester, when most hematopoietic websites disappear as the bone marrow develops. Throughout the third trimester and nicely through childhood, the liver microanatomy matures from the hilum outwards, with the final maturation of the parenchyma not being completed until the adolescent years. Portal tracts are the distribution network for the portal vein and hepatic arterial systems, and in turn the effluent assortment community for the biliary tree. The parenchyma is residence to hepatocytes, which account for 60% of the total cell population and 80% of the amount of the liver and are organized in an anastomosing system of plates that traverse the gap from the portal tract to the terminal hepatic venule. So-called nonparenchymal cells lining the sinusoid include: sinusoidal endothelial cells, perisinusoidal hepatic stellate cells, and intraluminal Kupffer cells. Lastly, blood flowing through the sinusoids exits the liver through the branches of the hepatic venous system, the smallest of which is the terminal hepatic vein (also termed the central vein, as shall be discussed). Terminal hepatic vein Terminal hepatic vein Portal Tracts and the Biliary System Both the portal vein and the hepatic artery, together with efferent autonomic nerves, enter the liver at the hilum. Branches of hepatic arteries also provide the peribiliary plexus of capillaries nourishing the bile ducts. Because all these vessels have independently contractile periarteriolar sphincters, the sinusoids receive a various mixture of portal venous and hepatic arterial blood. These veins course independently of the portal tracts and drain through the major hepatic veins, which emerge to join the inferior vena cava by way of separate orifices from the most important liver lobes. Lymphatic fluid originates from retrograde fluid move within the house of Disse and is thereby collected into blind-ended lymphatic capillaries in the connective tissue spaces throughout the portal tracts. The fluid contained in these lymphatics strikes toward the hepatic hilus and finally into the cisternae chyli and thoracic duct. Smooth muscle cells at strategic points in the vascular community create useful sphincters that contribute to local blood move regulation. Interconnections between the portal vein and hepatic artery networkalsoaredepicted. Lymphatics within the hepatic capsule drain to vessels both on the hilum or across the hepatic veins and inferior vena cava. These buildings had been originally thought to be seen solely by electron microscopy. The bile ductule connects with the terminal bile duct at a roughly perpendicular angle-on three-dimensional step sections the angle of intersection is barely off-perpendicular. The bile ducts converge down the size of the biliary tree, finally exiting the liver hilum as the best and left bile ducts to type the frequent hepatic bile duct just outdoors the liver corpus. Owing to regular variation in human bile duct anatomy, in 30% to 40% of people the confluence of the frequent hepatic bile duct is just internal to the liver. Given the limitations of retrograde filling methods, and uncertainty in whether or not the terminal biliary tree branches symmetrically (dichotomously) or asymmetrically, the exact geometry of the intrahepatic biliary tree remains conjectural. Regardless, the grownup liver must be supplied by four hundred,000 to 500,000 terminal bile ducts, comparable to the estimated 440,000 microarchitectural models (defined as lobules or in any other case, see later) estimated to exist in the adult liver. Bile acids resorbed by the biliary epithelium are recirculated to hepatocytes through the peribiliary capillary plexus, making a cholehepatic shunt pathway and selling bile acid�dependent bile circulate. Along with mucin, these glands secrete substances such as lactoferrin and lysozyme.
Home
| About MM Research, Inc. | Online
Publications © Copyright 1987-2011, MM Research, Inc. 5748 N. Camino del Conde, Tucson, Arizona 85718 |